
63-year-old male with history of 30-pack-year of smoking presented with cough. The chest CT showed 3.9 cm left upper lobe mass centered near the left hilum with extension into the left mainstem bronchus. Bilateral mediastinal lymphadenopathy and left supraclavicular lymph nodes enlargement were seen.
EBUS-guided FNA of level 4R lymph node was performed.
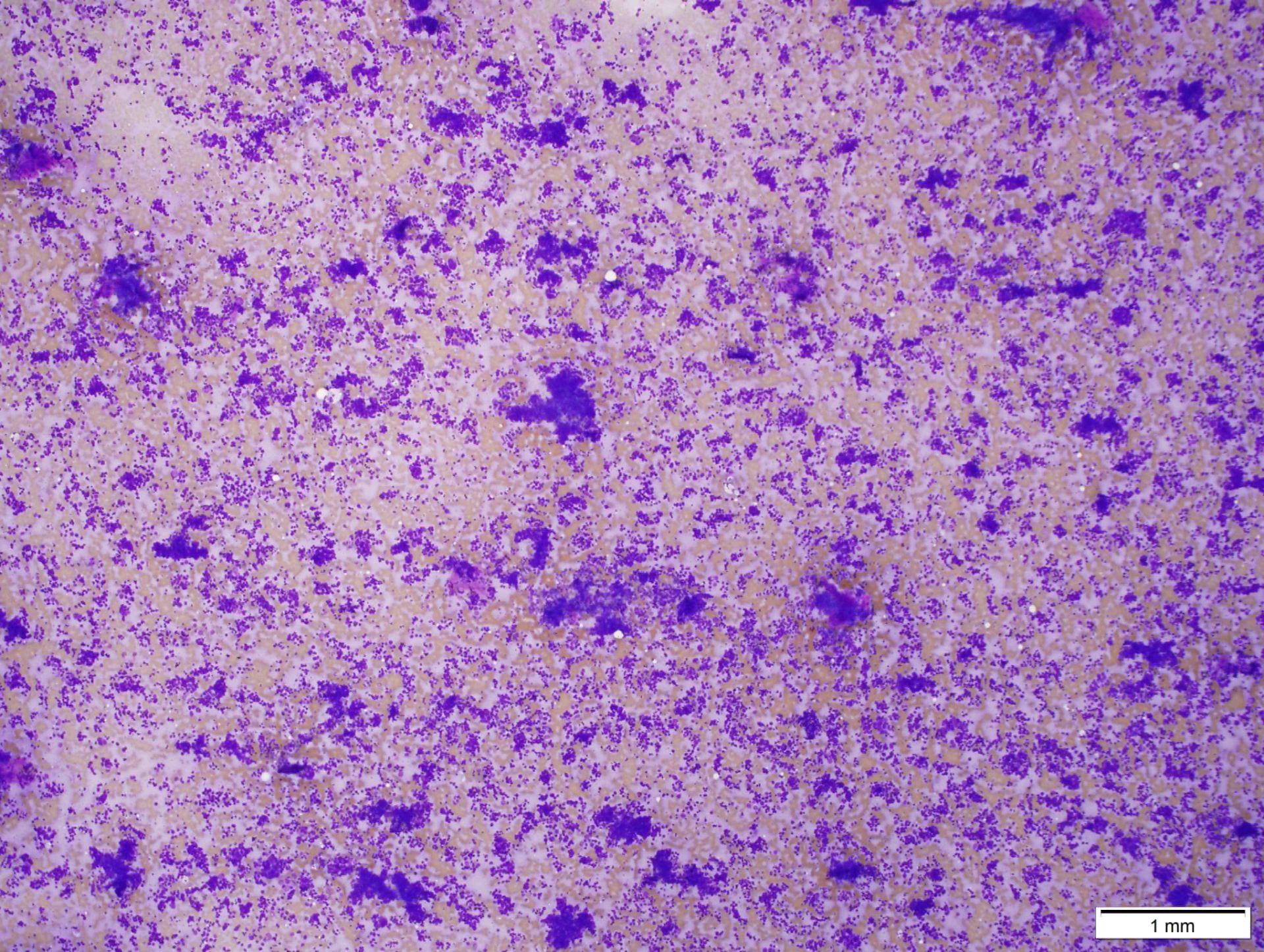
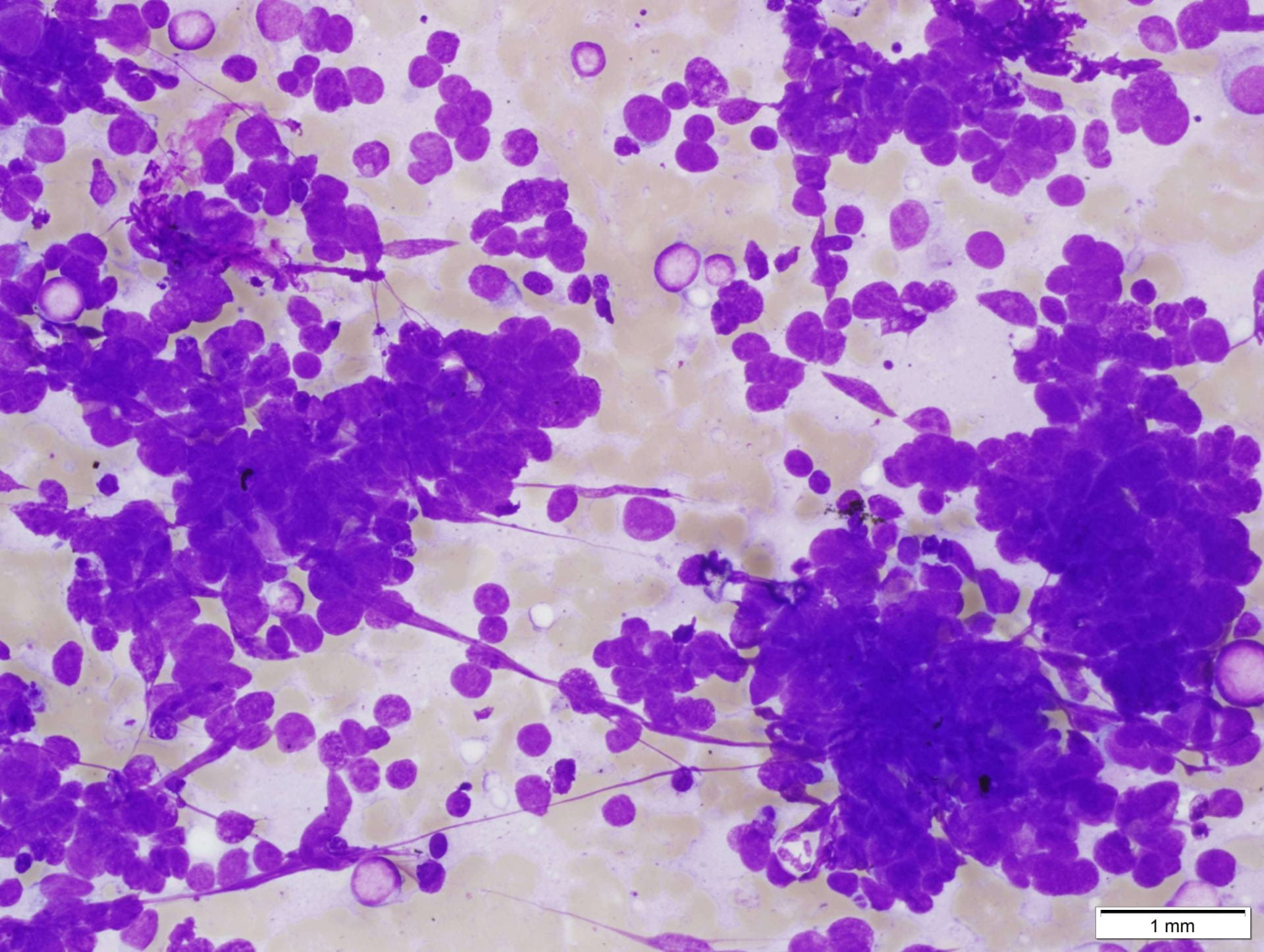
On Diff-Quik preparation, low power (4x) view is hypercellular. The tumor cells are loosely cohesive or forming small clusters. At high power (40x) magnification, the tumor cells are about 2 times the size of lymphocytes. They have high n/c ratio, very scant cytoplasm, round to oval nuclei, relatively smooth nuclear membrane, and inconspicuous nucleoli. Some cells show molding and crush artifacts. Abundant apoptotic bodies can be readily appreciated. Background of lymphocytes are present.
On Pap stained slides, at high power (40x) magnification, the tumor cells again are small (2 times the size of lymphocytes). They are either loose cohesive or aggregated into clusters with overlapping, molding and crush artifact. The cells have minimal cytoplasm, but round to oval and hyperchromatic nuclei, granular “salt-and-pepper” chromatin, and inconspicuous nucleoli. Mitosis and many apoptotic cells are readily seen. Lymphocytes are present in the background.
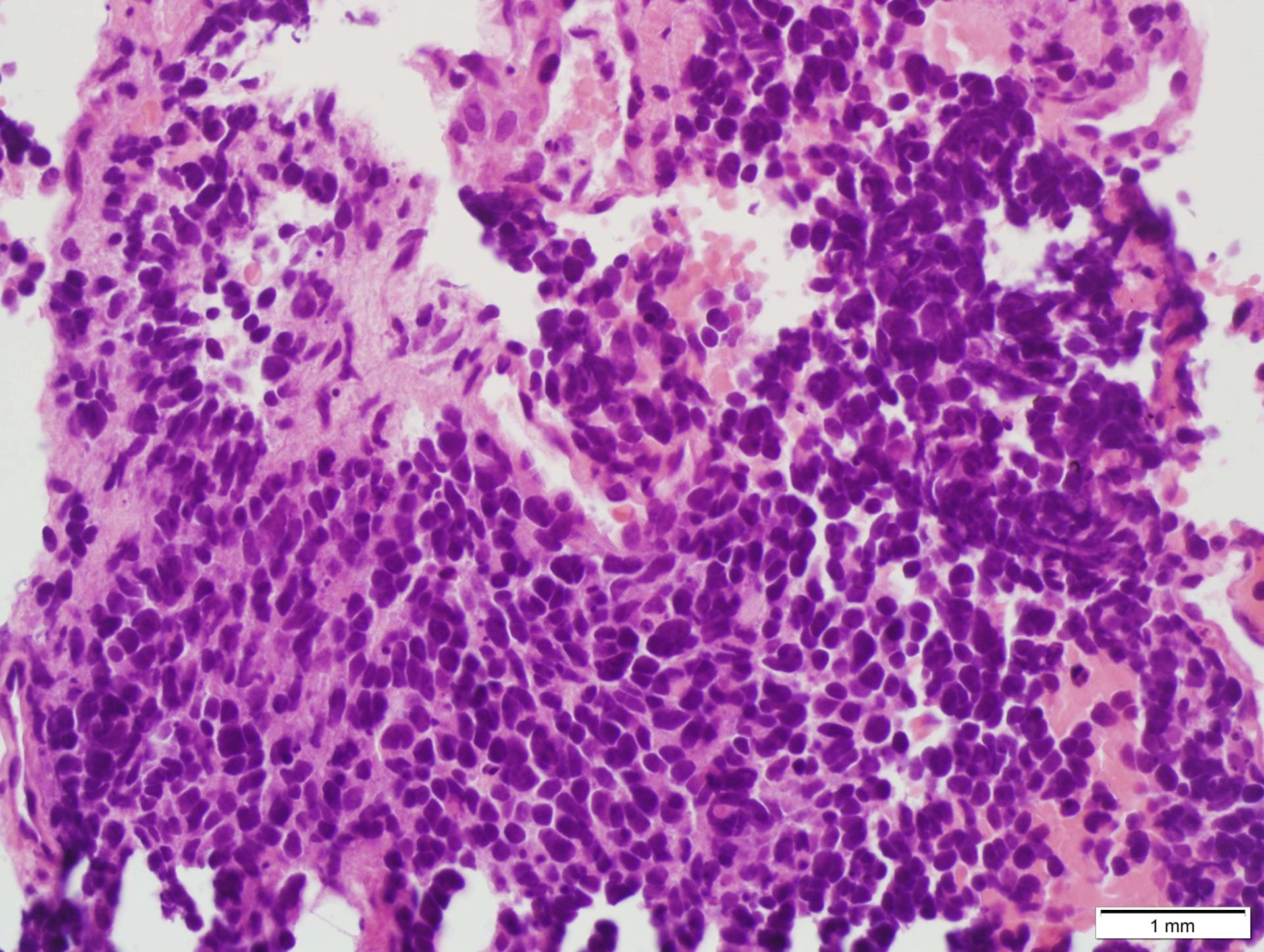
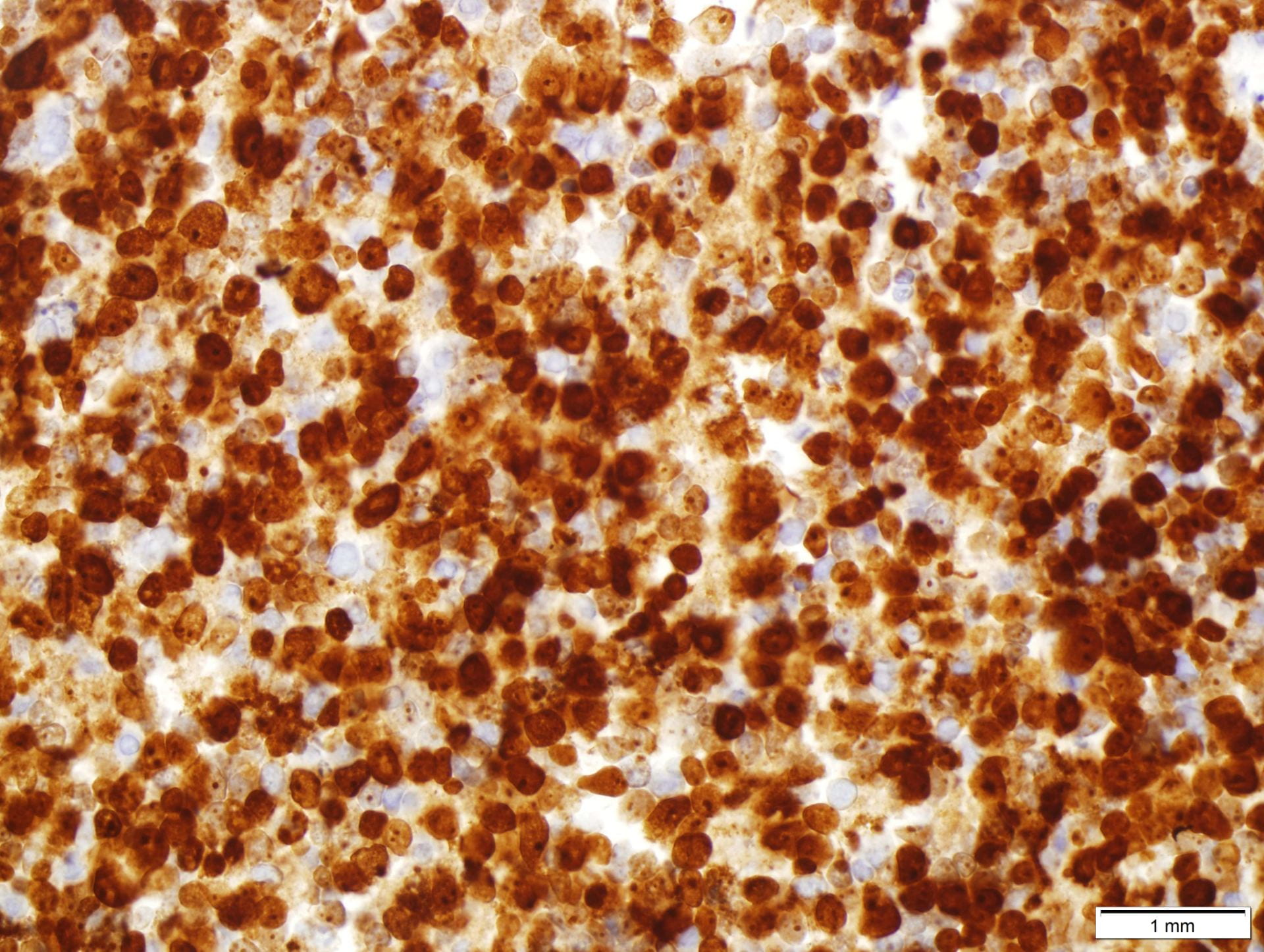
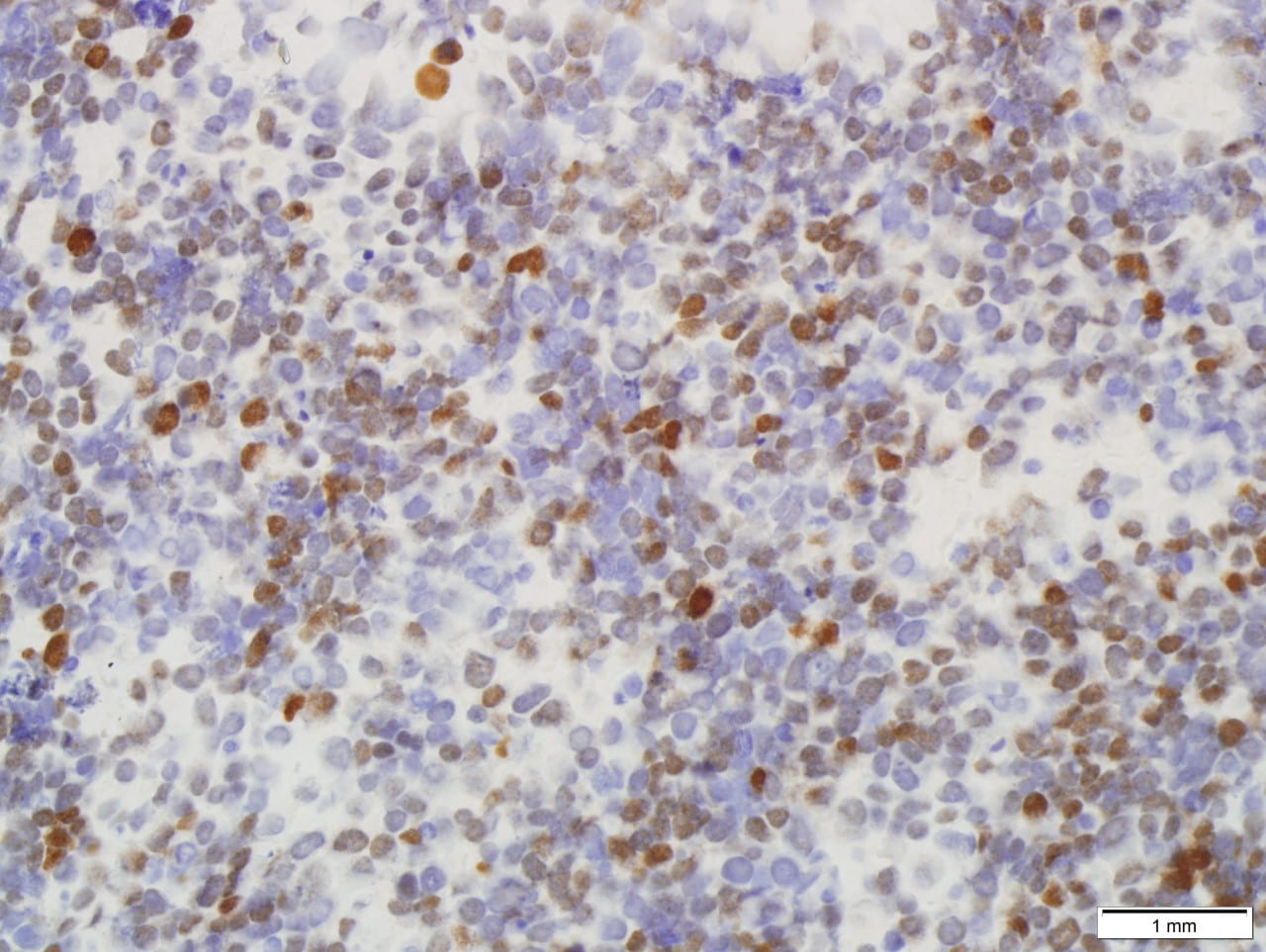
Cell block is hypercellular with marked crush artifacts. The small to medium sized, round to oval and hyperchromatic tumor cells show high n/c ratio, minimal cytoplasm, molding and smudging nuclei with finely dispersed chromatin, lack of distinct nucleoli. Apoptosis and mitosis are seen. Immunohistochemically, the tumor cells are moderately to strongly positive for TTF-1, strongly and diffusely positive for synaptophysin. Mitotic index of Ki67 is very high (greater than 90%).

Discussion: Pulmonary small cell carcinoma is a high-grade neuroendocrine carcinoma, accounting for 20-25% of all primary lung carcinomas. It is thought to be derived from Kulchitsky cells. Most patients are male smoker (80%). Patients usually present with rapid growing and metastasizing lung mass. Instead of surgical resection, the main treatment for small cell carcinoma is chemotherapy and radiation. The prognosis is very poor with months of the life expectancy
Principle cytologic features of small cell carcinoma include that the tumor cells average approximately 1.5-2 times the size of lymphocytes with scant cytoplasm, finely granular chromatin with a typical salt-and-pepper granular appearance, absent to inconspicuous nucleoli, nuclear molding, and associated apoptosis and mitotic figures. Immunohistochemically, the tumor cells show neuroendocrine markers including CD56, synaptophysin, chromogranin and INSM. TTF-1 is typically positive. Due to the minimal cytoplasm, pan-cytokeratin usually weak/focal or even negative.
Distinguishing between small cell carcinoma from poorly differentiated non-small cell carcinoma and lymphoma is important because of significant differences in patients’ management and prognosis. Lymphoid cells are typically discohesive or singly dispersed without forming cell clusters. Background of lymphograndular bodies is a helpful clue for lymphoid cells. Small cell carcinoma sometimes is difficult to distinguish from non-small cell carcinoma, particularly squamous cell carcinoma with basaloid features and adenocarcinoma. Finely granular chromatin, inconspicuous nucleoli, nuclear molding and crush artifact are useful features for small cell carcinoma. In difficulty cases, immunohistochemical panels include p40, neuroendocrine markers, Napsin A and TTF-1 will help.
References:
Cibas, ES; Ducatman, BS. Cytology: Diagnostic principle and clinical correlation (4th ed.)