
Clinical History
- The patient is a 45 y/o gentleman with PMHx of Non-Hodgkin’s Lymphoma in remission and significant tobacco use who presented to the emergency department with 1 week of worsening abdominal pain. The abdominal pain was described as sharp and radiating to the left flank.
- Initial lab work showed hypercalcemia with CT Abdomen and Pelvis showing a 10.2 cm mass in the tail of pancreas, diffuse retroperitoneal and mesenteric lymphadenopathy, inguinal lymphadenopathy, and a 3.0 x 2.9 x 2.3 cm solid mass in the right inferior thyroid.
- At the time, the thyroid mass was favored to possible represent a possible focus of metastatic carcinoma vs nodal disease vs primary thyroid lesion.
FNA of the thyroid nodule was planned and performed.
Cytology
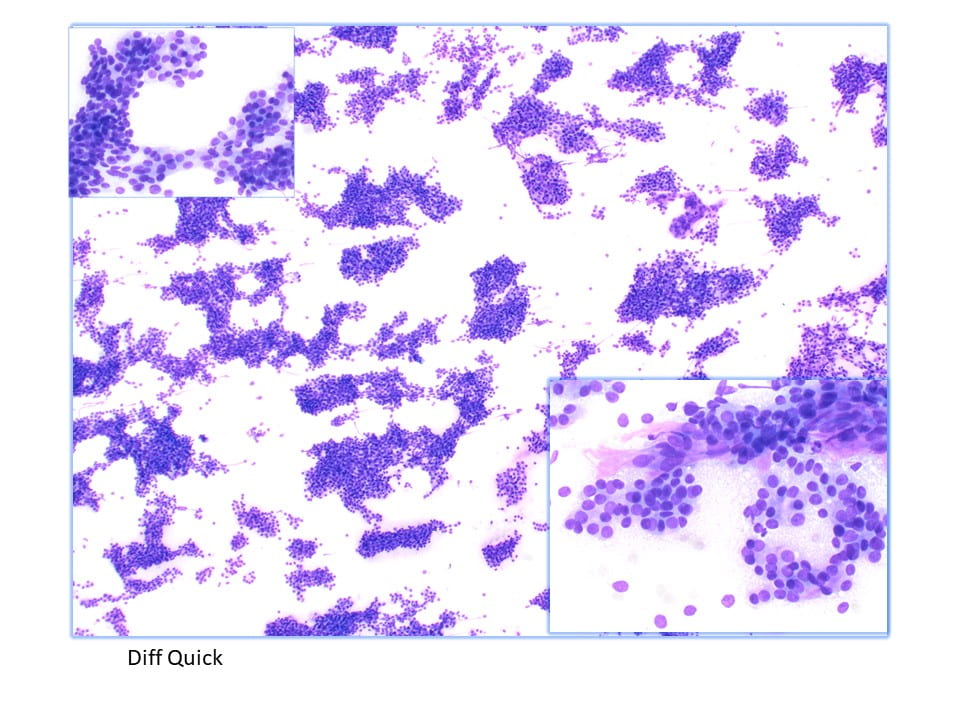
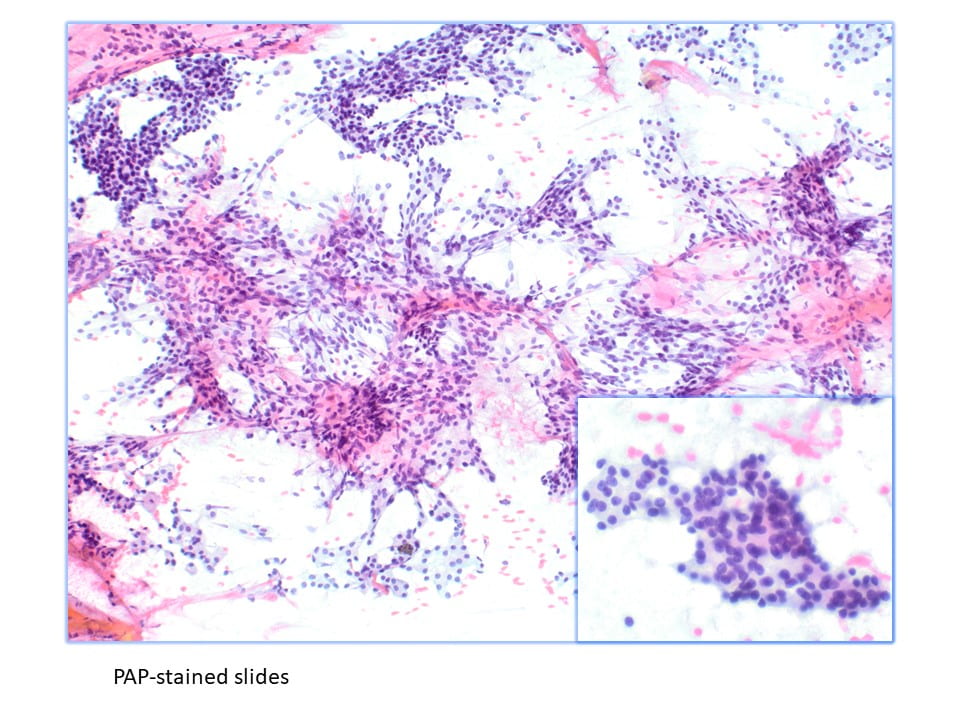
- The Diff-Quik and Pap-stained preparations were highly cellular, showingcohesive sheets, ribbon-like and corded structures, crowded trabeculae, and both macrofollicular- and microfollicular-like arrangements of cells with round to oval nuclei, mild anisonucleosis, granular chromatin, small and conspicuous nucleoli and moderate amounts of fine cytoplasm. There were admixed inflammatory cells, single and dispersed and naked nuclei and anucleated squamous in a bloody background. Although somewhat less cellular, the cell block showed similar findings.
-
The initial differential diagnosis included a follicular neoplasm, metastatic adenocarcinoma, and sampling of the parathyroid gland.
![]()
Diagnosis
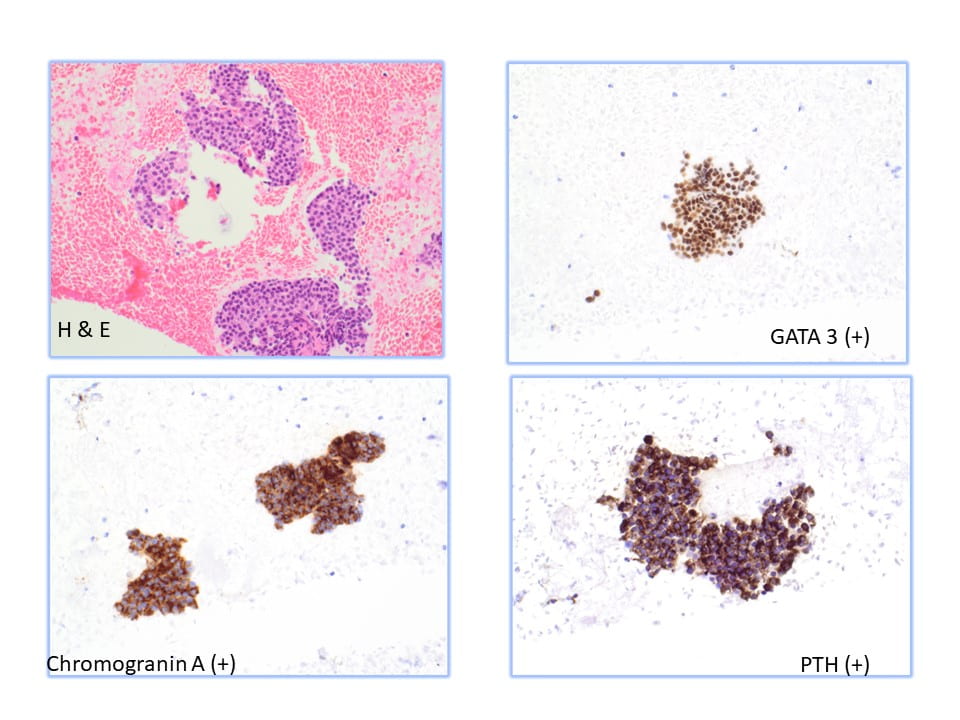
- The histomorphology and immunohistochemical findings from the left thyroid FNA best fit as hypercellular parathyroid tissue, with a differential diagnosis of hyperplasia vs neoplasm with clinical correlation required for distinction.
Discussion
Parathyroid tissue on FNA can be difficult to identify due to overlapping features with thyroid neoplasms, particularly follicular neoplasms. Parathyroid tissue has been misdiagnosed as follicular thyroid carcinoma, papillary thyroid carcinoma, and medullary thyroid carcinoma on FNA. The sensitivity of FNA in the diagnosis of parathyroid tissue has been reported to be between 40% and 86%. The previous literature regarding FNA of the parathyroid gland has only characterized the cytomorphology on FNA smears. Characteristics such as high cellularity, the presence of naked nuclei, loose 2-dimensional clusters, and papillary architecture on FNA smears are suggestive of parathyroid tissue.
- Ultrasound has no specific findings to distinguish parathyroid, thyroid, and lymph nodes.
- Serum PTH level or hypercalcemia can be used as an important clue.
- Overall, Parathyroid FNAs show intermediate-to-high cellularity, occasional papillary fragments, tight clusters, and microfollicular patterns with numerous naked nuclei in background.
- They tend to have more stippled/hyperchromatic nuclei than thyroid follicular cells.
- Bethesda IV tends to have more prominent nucleoli.
- Anisonucleosis also tends to suggest Parathyroid as opposed to Bethesda IV.
References
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5430501/
- https://pubmed.ncbi.nlm.nih.gov/19283690/
- Cibas, Edmund S., and Barbara S. Ducatman. Cytology: Diagnostic Principles and Clinical Correlates.Elsevier, 2021.